The first report of a strange new heart disease began in 1990, among the chaos and carnage of a huge earthquake in Japan. Hospitals were inundated, not only by the injured from the earthquake damage, but also a wave of people with suspected heart attacks. This is a phenomenon that had been seen before around the time of major disasters and yet the cause had remained a mystery. But the difference from other such disasters is that it was happening in Japan, a country with a significant number of high-tech hospitals.
In Hiroshima City Hospital, doctors were now using state-of-the-art imaging techniques such as coronary angiography to visualize the coronary arteries—the blood vessels that supply blood to the heart muscles. Cardiologists inject a contrast agent to see whether there is a blockage from a clot or ruptured plaque that might be obstructing the vessels and causing the heart attack. But in a new procedure, they also moved the injection of contrast to the ventricle to show the shape of the heart as it contracts. In one group of patients, they saw two things that amazed and puzzled them.
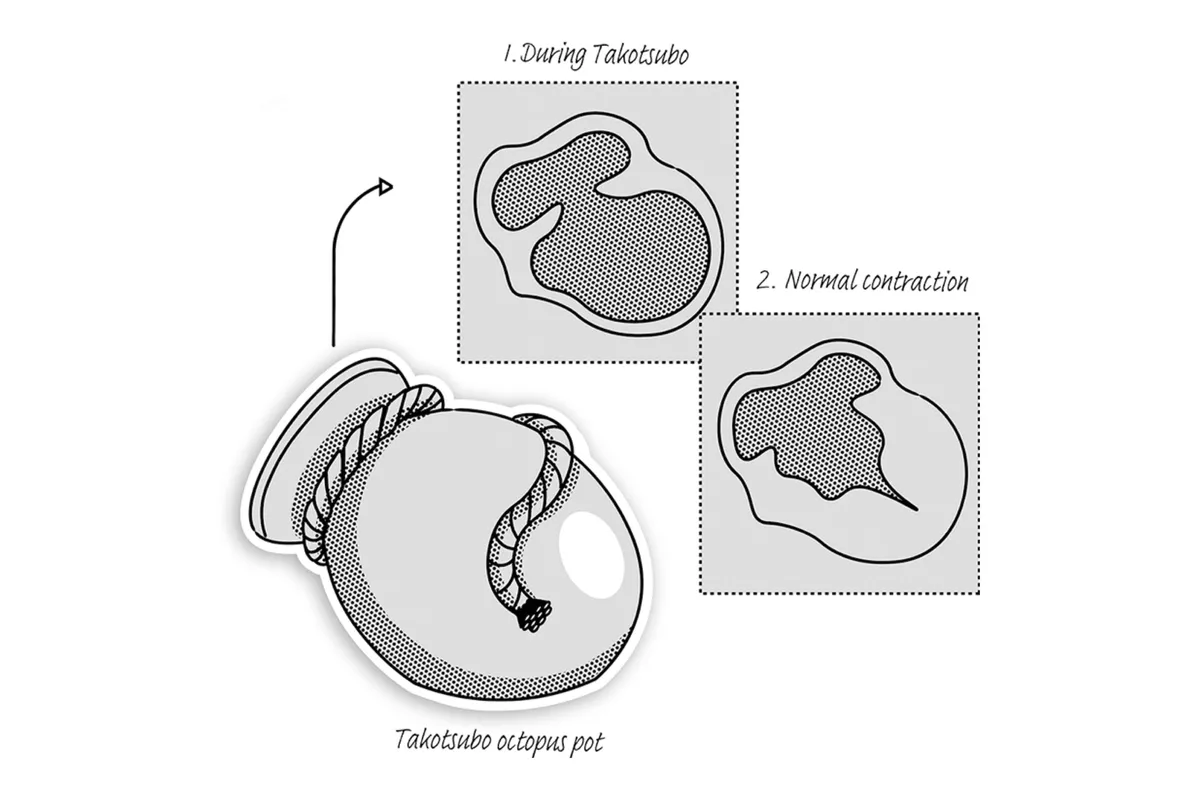
First, there was no blockage, despite the patient having all the pain, ECG changes, and blood markers that point to a heart attack. Second, the heart as it contracted showed a shape they had never seen before. The top of the heart near the atria (called the base) was contracting extremely vigorously, so much so that it was even blocking the outlet of the left ventricle. But the bottom of the heart (or apex) was almost immobile. This produced a shape like a balloon on the X-ray (see figure, below) or like a narrow-necked pot. It reminded the Japanese doctors of the pots, or takotsubo, used for trapping octopus. The narrow neck imprisons the creature after it crawls in. This has given the disease the eye-catching name of Takotusbo syndrome, also sometimes called stress cardiomyopathy, and it is the second broken heart syndrome.
Two other features made this syndrome stand out to the clinicians treating these patients. The first was that their patient group was mainly women. That’s quite unusual for heart disease in general, which is more expected in men—at least for younger or middle-aged people. In all age groups, the men outnumber the women, by more than two to one in ages below 64 years. It is true that the gap narrows in later life, after menopause, and in fact many of the women with Takotsubo syndrome were postmenopausal. When we add up the figures over many studies, an astonishing 80 – 90 per cent of patients in the Takotsubo group are women. This is a huge majority and one that had never been seen for a type of heart disease before.
An even more striking feature is that many of them recovered completely, with no sign of cardiac damage. They went from an emergency admission with severe chest pain and acute heart failure, to walking out of the hospital disease-free, sometimes in a matter of days. Most never had a problem again. To scientists and doctors, this is highly intriguing. We know people with this severity of acute heart failure would usually have a very poor outlook. If the cardiologists had not seen the strange shape of the heart and its bizarre contraction on the X-ray, then we would have thought that the patients had been imagining or misinterpreting the symptoms.
It’s very sobering, in fact, to think that women suffering from Takotsubo syndrome might have been dismissed as malingerers before such imaging was possible. You can see how a middle-aged woman, distraught after an upsetting event, coming into the hospital with chest pain and collapse but recovering quickly, might have been seen as having a “hysterical” illness.
Taking this even further, many people who have panic attacks say, “I thought I was having a heart attack, but I was fine after a while.” Maybe they were Takotsubo sufferers too?
Takotsubo - A new broken heart syndrome
The classic Takotsubo syndrome patient is a woman in her 60s. Let’s call her Mary. She is active and sociable with a wide circle of friends who lean on her for advice. She has a close but complicated family: maybe her grown children are divorced, and she is helping with the grandchildren. More often now she is shuttling back and forth to look after elderly parents while perhaps juggling a job, too. Her days are busy and draining. She certainly doesn’t think much about her own health, dismissing aches and pains as the inevitable part of oncoming age. Her husband is her rock and comfort in all her troubles, and they have supported each over the problems of the years.

Then her world falls apart. Her husband dies: maybe suddenly, with no time to say goodbye, or maybe after she has nursed him through a long and difficult illness. The funeral arrangements go past in a blur; she is in a kind of numb shock. Her thoughts are for her children and grandchildren, to comfort them in their distress.
During the funeral or the following days, she feels increasingly unwell. At first, she doesn’t notice how bad she feels against the background of her grief and sorrow, but as the rush dies down the exhaustion and nagging chest pain get worse. She soldiers on, not wanting to cause her family any trouble, hoping that the feelings will subside. She may collapse, or finally admit how awful she feels, and is taken by her worried family to the hospital. Thankfully, this facility has doctors who take her symptoms seriously and act rapidly.
Doctors know that “time is muscle,” and saving heart muscle has a profound effect on the future lifespan and quality of living for the patient. Highly sophisticated imaging is now common. Fewer people are dying, and many get back to a good quality of life. Mary is quickly taken to the ER and the doctors see that her ECG and symptoms ring alarm bells that point to a possible heart attack. They take her to the catheter laboratory to give her an angiogram, where the blood vessels are visualized by a live X-ray during which a contrast agent is injected into the coronary arteries.
What they are looking for is the culprit blood vessel that has been blocked by a blood clot or an atherosclerotic plaque (a thickening of the vessel wall containing cholesterol) that has suddenly burst. The cardiologist does not see any blockage, but there is not a great deal of surprise. This does happen—maybe the clot has broken up or the blockage was due to the blood vessel having a spasm. However, the bizarre motion of the heart alerts them to something very different happening, and the weak contraction of the apex is a real concern.
What happens next actually depends on whether the doctors have heard of Takotsubo syndrome. Knowledge is spreading, but while hospitals in major cities are experts in a wide variety of heart conditions, including this one, smaller local hospitals may have seen only a few Takotsubo cases. In this hospital, they are unsure of what to do. Mary is put under observation while they decide and give supportive care that keeps her condition stable. Now that the emergency has subsided, they can take some time. Mary begins to feel better over the next few days, so she has cautiously begun walking about the ward.
A week or so later she is examined again, and her heart is functioning better, although not completely normally. The pattern of apex/base difference is not so evident. Mary has been lucky: a small percentage of Takotsubo victims die of complications during the acute first illness, but like most others, she has passed through the immediate danger and the prognosis is good.
Another week passes, and the improvement continues. Mary is longing to get home and protests that she feels “fine”; meanwhile, new patients are lining up for her bed. She is discharged and goes back to her busy life with support and care from her family. Months later she comes for another check-up. Her heart is functioning adequately – not like a 20-year-old, but not so unusual for her age. The doctors chalk this one up to experience, just happy that the outcome was good.
Of course, no one had examined her before the attack, so there is no way of knowing whether she has truly recovered completely. She feels okay, with less energy and enthusiasm for life than before but, well, that’s to be expected after losing her husband.
Has she really recovered completely? It’s difficult to tell.
Who will get takotsubo?
Takotsubo syndrome is relatively rare – of all the people who come to the ER with a suspected heart attack only about 3 per cent turn out to have this syndrome. We suspect the true rate might be a bit higher, since it is not universally well diagnosed because of the variation in the syndrome, but it is still a low percentage. If you have underlying heart disease or a certain type of mutation, there can be an increased risk of SCD. But is this also the same for Takotsubo?
It is true that the risk of a second Takotsubo attack is high in sufferers who have already had one, with around 10–15 per cent experiencing another one. This points to some underlying factors predisposing people to the syndrome, separate from the final adrenaline surge. Take our case of Mary: her heart function was found to be moderately impaired after the episode, but this could have been something she had been living with for a while. Perhaps this made her more likely to have an attack? There has been a search for a mutation that could link to Takotsubo, but nothing very conclusive has turned up. We do have a clue, however, that another class of molecule, which controls how genes turn on and off, might play a role in Takotsubo. These are the microRNAs—the orchestral conductors of the body.

When the human genome was first sequenced in 2001 it was a surprise to everyone how few genes there were (20,000— which is fewer than a water flea has) and how much of the genome (more than 90 per cent) didn’t code for any genes. Because this noncoding region would not produce any of the proteins in the cell, it was known first as junk DNA and thought possibly to be left over from viruses that had infected us. But much of this is far from being junk DNA. We now know for example that the microRNAs, short sequences copied from the DNA, come from part of this noncoding DNA. MicroRNAs act to turn on and off groups of genes quickly and flexibly, to orchestrate responses to the challenges of daily life.
When Takotsubo syndrome was first identified, clinicians looked for ways to identify Takotsubo patients and distinguish them from others having heart attacks. This was important because some of the drugs or tests for heart attacks, like dopamine stress testing, would make the Takotsubo patients worse. Two microRNAs, it turned out, were clearly raised in the blood of Takotsubo patients but not in the heart attack victims and so were “biomarkers” for the syndrome.
We gave these to our rats for several weeks and found that they would switch to the depressant response much more easily. They had been primed to get Takotsubo. The two microRNAs are linked to anxiety and depression: for example, students going through the stress of exams show raised levels of these molecules. Turning back to Mary, our Takotsubo sufferer, it is possible that her complicated life and day-to-day stress had made her susceptible, so that when the adrenaline surge finally came, she was more likely to get Takotsubo.

What's next for the takotsubo patient?
First, do no harm
By now, we have at least learned what not to do for the person diagnosed with Takotsubo syndrome. No adrenaline, no indirect beta-receptor stimulants, no dobutamine stress test. Possibly some stimulants unrelated to the beta-receptor might work—these help in the rat but need to be tested in people.
However, the sudden and rare occurrence of Takotsubo makes a planned clinical trial very difficult to organize. Blocking the microRNAs might be a good pretreatment but, first, this kind of drug is only just coming onto the market and second, we would have to give it to many thousands of people just to protect the susceptible ones.
The same thing is true for beta-blockers, which could prevent the effect of the adrenaline surge but would have to be taken by many apparently healthy people. It would be ideal if we could predict the people likely to react to high adrenaline with an extreme response, so that we could protect them with these drugs.

So, our plan is to screen as many people as possible for a Takotsubo-type pattern of cardiac function. We will start with people who have one attack, since we know they are more likely to have another. Our study will equip them with wrist monitors, like Fitbits and Apple watches, to record heart rate variability and physical signs of stress. Patients will also record when they are stressed in a diary app.
We will look for patterns of high sensitivity to adrenaline (the trigger) followed by an anomalous dip in cardiac function (the signalling switch). We will use these patterns (and with artificial intelligence methods look for others that we would not have predicted) to link them to Takotsubo recurrence.
Eventually, we will roll this out to volunteers to see if our idea is right that most people will show this effect to some extent, and that maybe it is part of the physical symptoms of anxiety and panic attacks. Hopefully, we can use the apps to help sufferers to understand their susceptibility and to anticipate and avoid another attack. Maybe it will also be a comfort to know that, ultimately, it is part of a natural mechanism to protect us from the risks and dangers of adrenaline.
The Exquisite Machine ($28.95, The MIT Press) is out now and is available from these outlets and Amazon UK.
Read more:
